Call us now
08045813058
FIBER OPTIC LARENGOSCOP

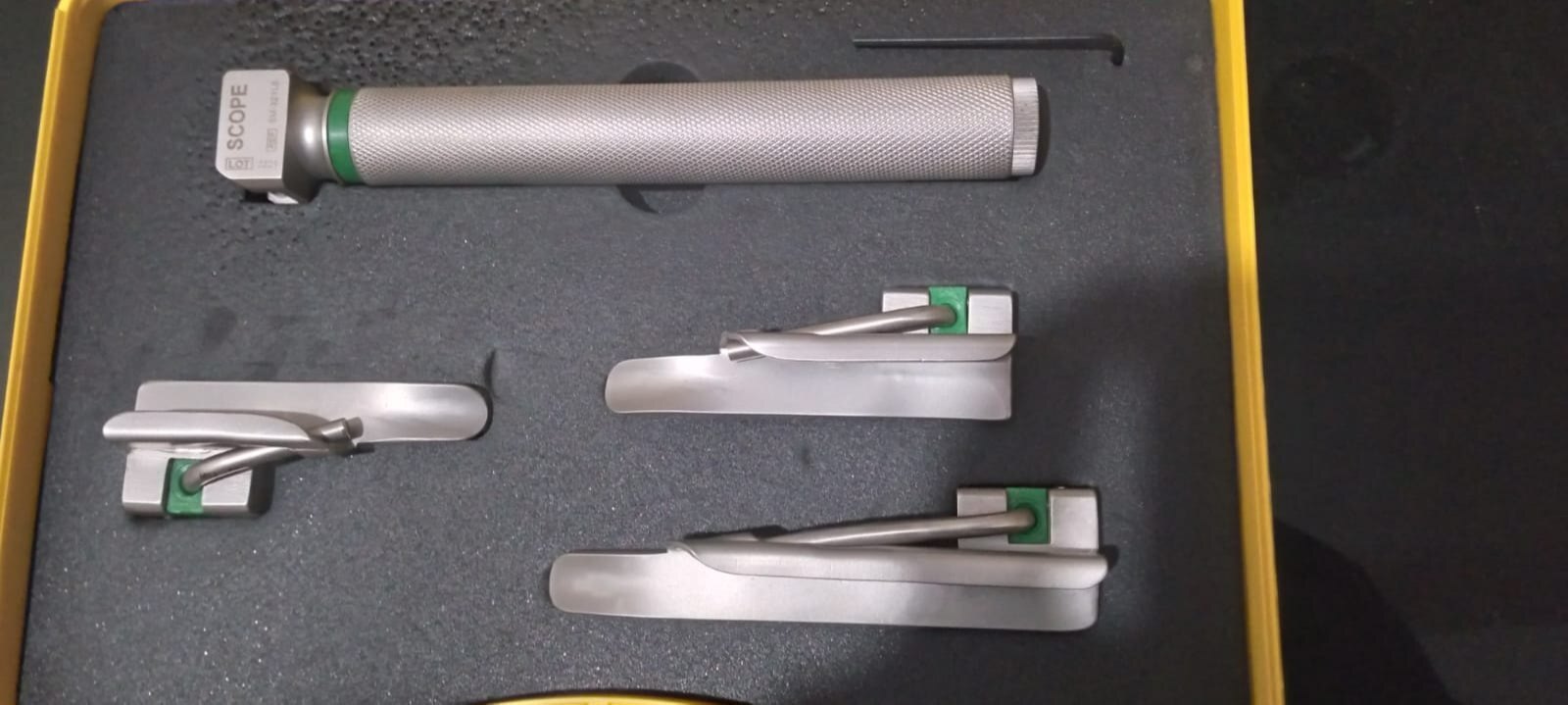
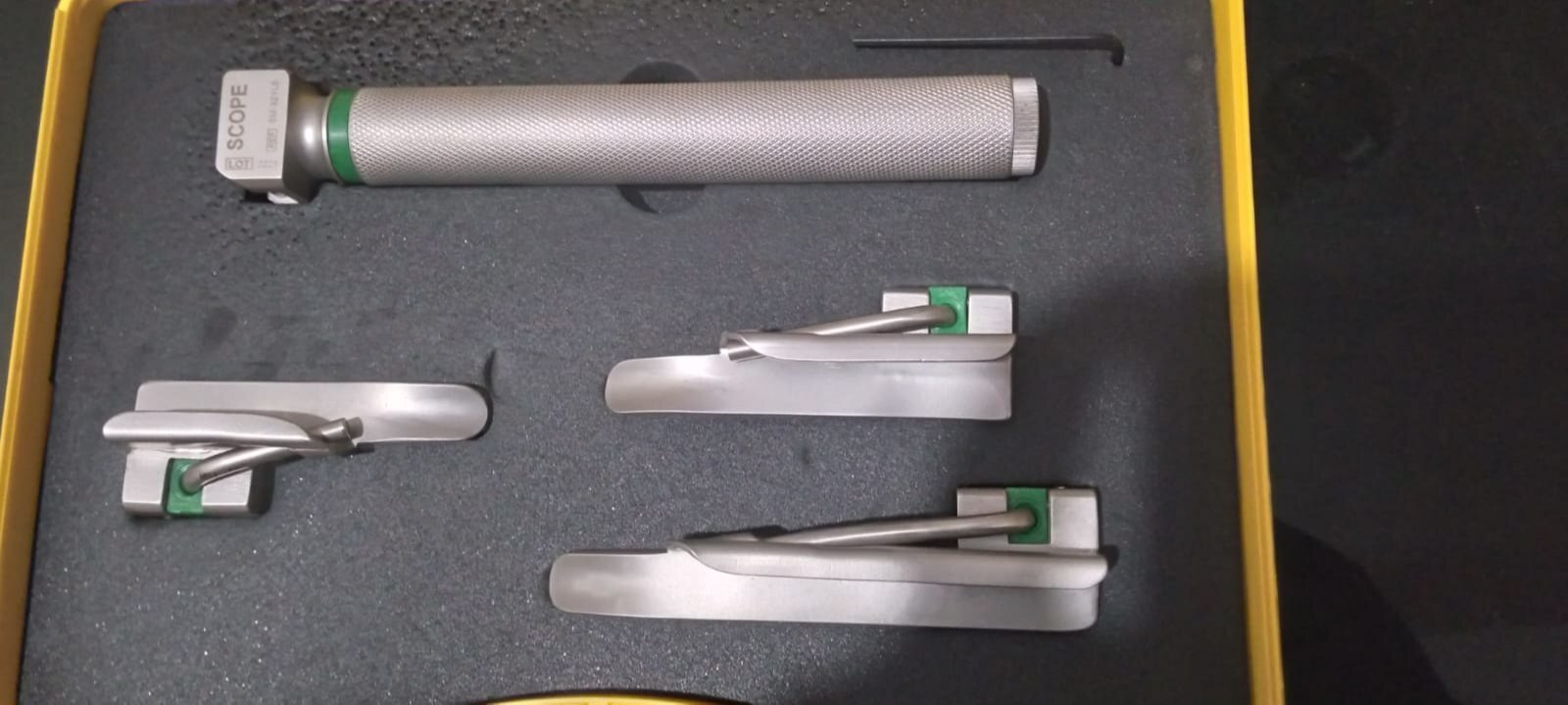
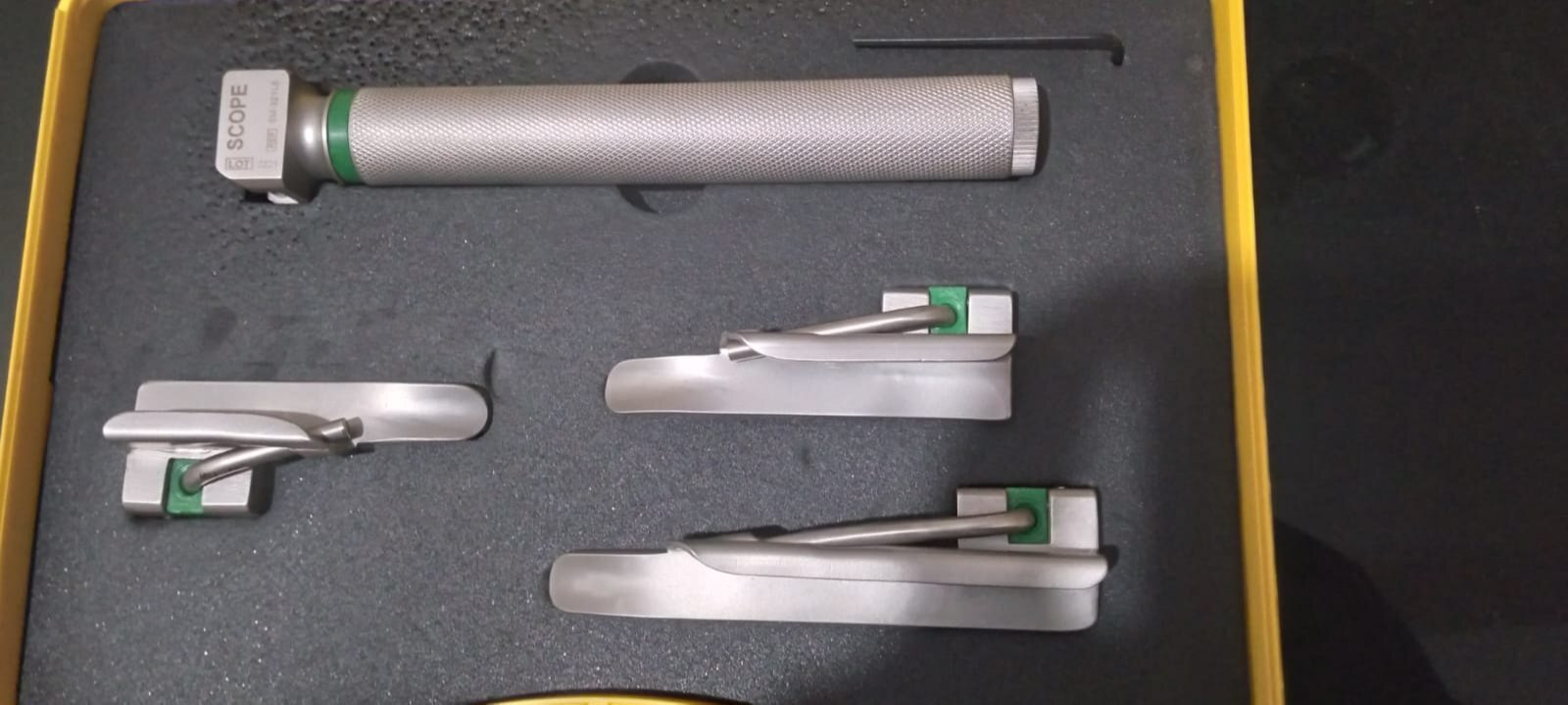
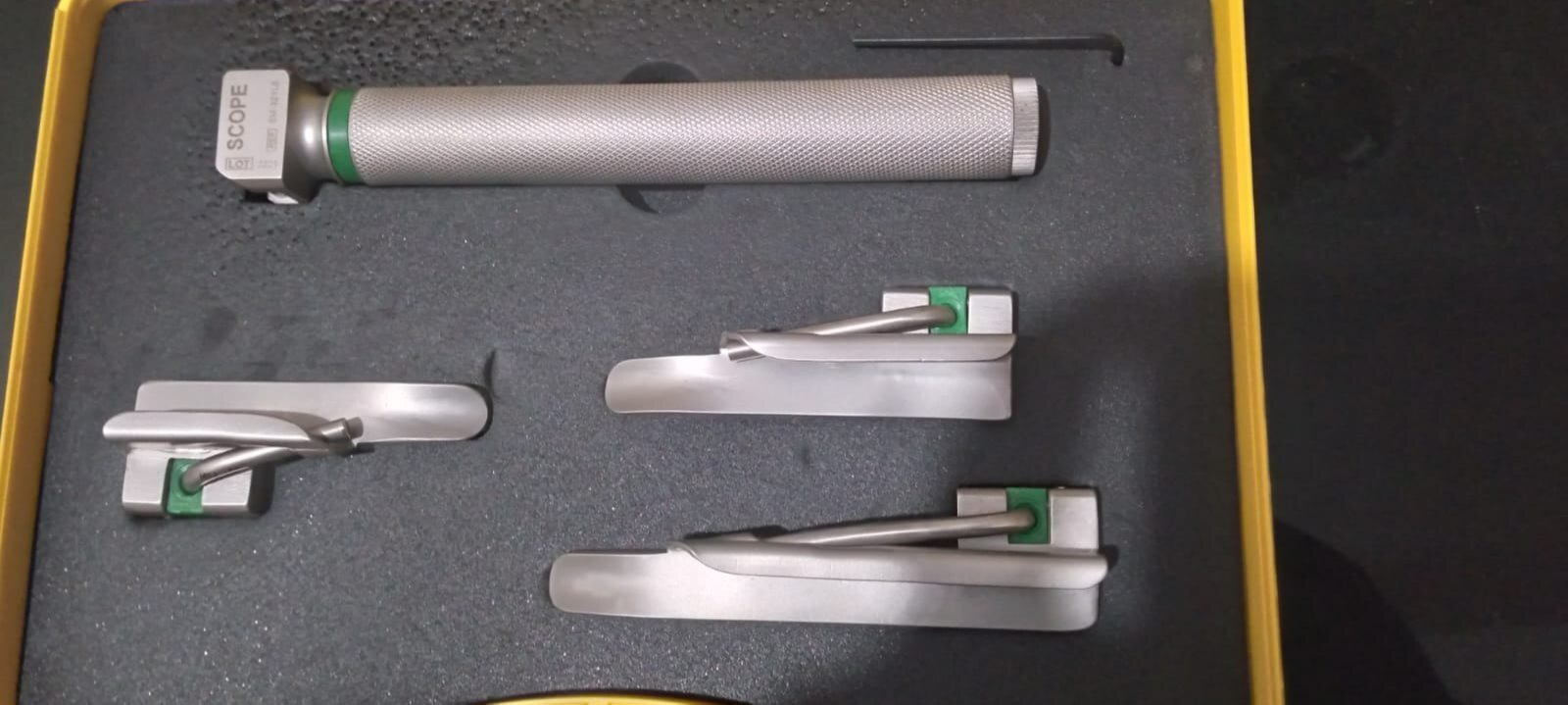
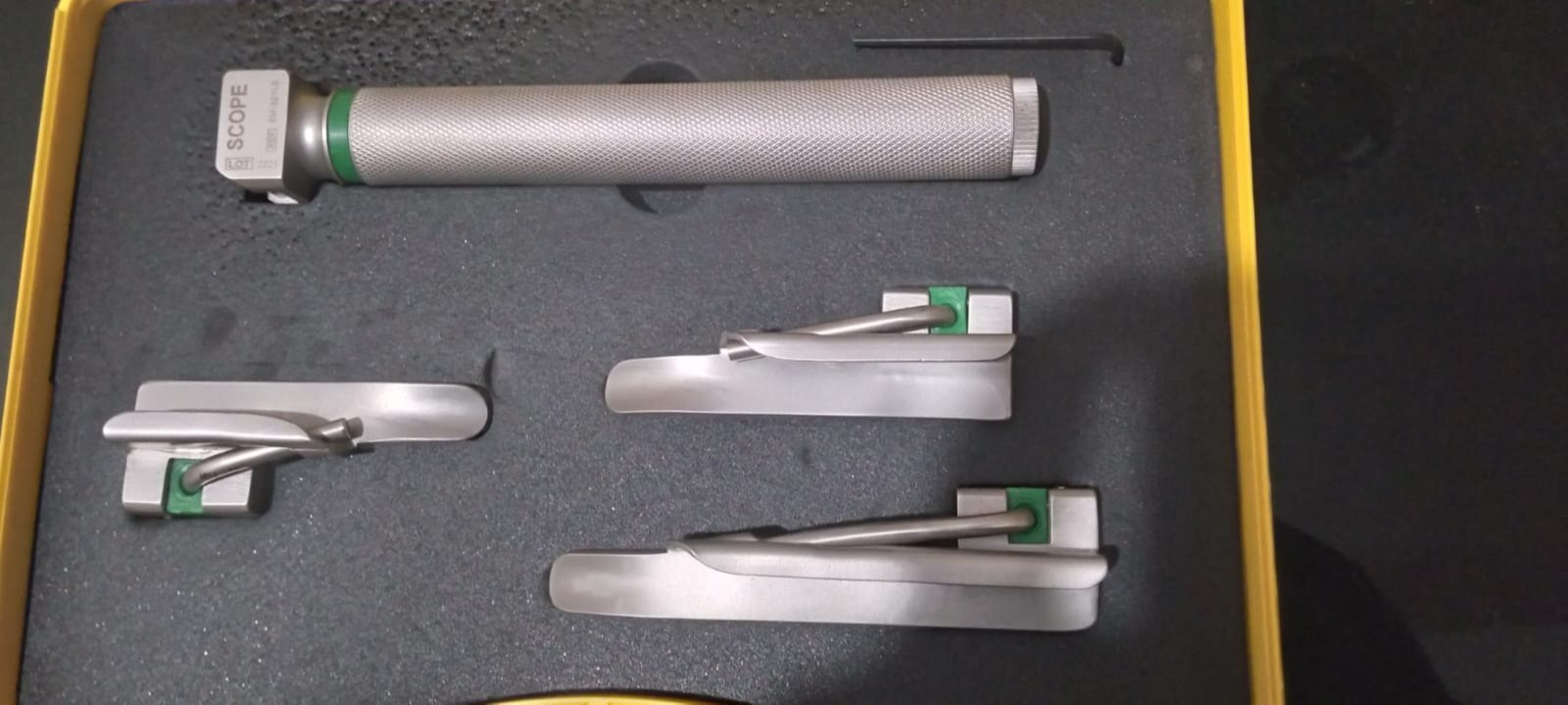

FIBER OPTIC LARENGOSCOP Specification
- Storage Instructions
- Store in Clean, Dry Place
- Function
- Direct Visualisation of Larynx
- Display Type
- No Display
- Instruments Type
- Surgical Instrument
- Usage Type
- Reusable
- Accuracy
- High Visualization Clarity
- Features
- Removable Blades, Autoclavable, Anti-rust, High Illumination
- Shelf Life
- Long
- Equipment Type
- Fiber Optic Laryngoscope
- Material
- Stainless Steel and Medical Grade Plastic
- Condition
- New
- Technology
- Fiber Optic Illumination
- Portable
- Yes
- Wall Mounted
- No
- Real-Time Operation
- Yes
- Noise Level
- Silent Operation
- Operating Type
- Manual
- Use
- Endotracheal Intubation, Airway Management
- Power Source
- Battery Operated
- Power Consumption
- Low
- Voltage
- 1.5V (battery)
- Dimension (L*W*H)
- Standard Blade Sizes, Handle: Ergonomic Length
- Weight
- Lightweight
- Color
- Silver (Handle), Green (Blade Attachment)
- Blade Types
- Macintosh and Miller Blades Compatible
- Handle Type
- Knurled, Non-slip Surface
- Corrosion Resistance
- Yes
- User Group
- Doctors, Emergency responders, Anaesthesiologists
- Blade Sizes Available
- 0, 1, 2, 3, 4 (Neonatal to Adult)
- Blade Material
- Fiber Optic Enhanced Stainless Steel
- Light Source
- LED or Xenon Bulb
- Handle Battery
- Standard AA or Rechargeable
- Sterilization Method
- Autoclavable up to 134°C
- Latex Free
- Yes
About FIBER OPTIC LARENGOSCOP
Direct laryngoscopy is carried out (usually) with thepatientlying on his or her back; the laryngoscope is inserted into themouthon the right side and flipped to the left to trap and move thetongueout of the line of sight, and, depending on the type of blade used, inserted either anterior or posterior to theepiglottisand then lifted with an upwards and forward motion ("away from you and towards the roof "). This move makes a view of theglottispossible. This procedure is done in an operation theatre with full preparation for resuscitative measures to deal with respiratory distress. There are at least ten different types of laryngoscope used for this procedure, each of which has a specialized use for the otolaryngologist and medical speech pathologist. This procedure is most often employed by anaesthetists for endotracheal intubation under general anaesthesia, but also in direct diagnostic laryngoscopy with biopsy. It is extremely uncomfortable and is not typically performed onconsciouspatients, or on patients with an intactgag reflex.Superior Fiber Optic Illumination
Engineered with advanced fiber optic technology, this laryngoscope delivers clear, high-intensity illumination for precise visualization during airway management procedures. The LED or Xenon light sources ensure consistent brightness and clarity, enhancing patient safety by assisting rapid, accurate intubation in critical scenarios.
Versatile Blade Compatibility and Sizing
This laryngoscope supports both Macintosh and Miller blade types, accommodating sizes 0 through 4. From neonatal to adult patients, practitioners can quickly select and attach the appropriate blade, making the instrument suited for diverse clinical settings and patient needs.
Robust, Portable, and User-Friendly Design
With an ergonomic, knurled handle and lightweight build, the device prioritizes comfort and control during use. It remains portable and operates silently, ideal for fast-paced or emergency environments. The non-slip surface and corrosion-resistant materials maintain long-term reliability with minimal maintenance.
FAQ's of FIBER OPTIC LARENGOSCOP:
Q: How do I select the appropriate blade size and type for different patients?
A: Choose Macintosh or Miller blades based on patient anatomy and clinical need. The available sizes (0, 1, 2, 3, 4) cover neonatal to adult patients, allowing you to match the blade size to the patient's age and airway dimensions for optimal visualization and intubation.Q: What is the process for sterilizing this Fiber Optic Laryngoscope?
A: The laryngoscope and its removable blades are autoclavable up to 134C. To sterilize, disassemble the device, clean all components, and place them in an autoclave as per standard protocols. Ensure the equipment is thoroughly dried before reassembly and storage.Q: What type of batteries are compatible with the handle, and how long do they last?
A: The handle operates with standard AA batteries for convenience, or you may use rechargeable counterparts to reduce waste. Battery life depends on usage and light source type, but the device is engineered for low power consumption and extended use.Q: Where should the Fiber Optic Laryngoscope be stored when not in use?
A: Store the instrument in a clean, dry area, away from direct sunlight or extreme temperatures. Proper storage helps maintain the device's performance, prevents corrosion, and ensures long-term durability and readiness for critical use.Q: What are the main benefits of using a fiber optic laryngoscope over standard models?
A: Fiber optic laryngoscopes provide brighter, focused illumination, offering improved visualization of the larynx for accurate intubation. The ergonomic design, compatibility with various blades, and autoclavability further enhance safety, efficiency, and user comfort.Q: When is it recommended to use this device in clinical practice?
A: Use this laryngoscope for direct visualization of the larynx, primarily during endotracheal intubation and airway management in hospitals, emergency responses, and surgical anesthesia settings. Its versatility and adaptability make it suitable for routine and emergency situations. Get Latest Price
Get Latest PriceTell us about your requirement

Price:
Quantity
Select Unit
- 50
- 100
- 200
- 250
- 500
- 1000+
Additional detail
Mobile number
Email

More Products in Intubation Devices And Accessories Category

MERIT MAP 152
Price 2000 INR / Piece
Minimum Order Quantity : 10 Pieces
Material : Other, ABS Plastic, Metal
Use : Hospital, ICU, Clinical, Emergency
Color : White & Grey
Condition : New

GANIOMETER STEEL INSTRUMENT
Price 1250 INR / Piece
Minimum Order Quantity : 10 Pieces
Material : Other, Stainless Steel
Use : Angle Measurement
Color : Silver/Grey
Condition : New

DISPOSABLE AUTOFILL HUMIDIFICATION CHAMBER
Price 1950 INR / Piece
Minimum Order Quantity : 10 Pieces
Material : Other, Medicalgrade polycarbonate, silicon gasket
Use : Maintaining humidified respiratory gases in ventilator circuits
Color : Transparent with blue caps
Condition : New
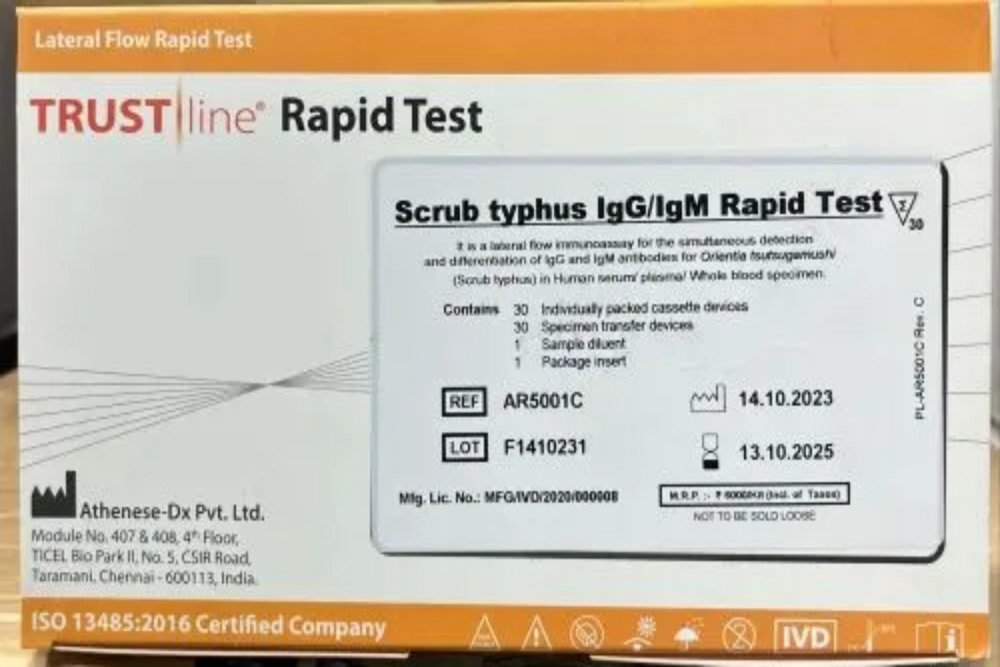
CTK TRUSTLINE SCRUB TYPHUS RAPID TEST CARD
Price 3000 INR / Piece
Minimum Order Quantity : 10 Pieces
Material : Other, Plastic, Paper, and Membrane components
Use : Detection of antibodies to Orientia tsutsugamushi
Color : White card with colored line indicators
Condition : New
Mark Enterprises
GST : 09CGDPG2368E1ZJ
GST : 09CGDPG2368E1ZJ
56/A, Gali No-3, Jai Bharat Enclave, Sahibabad, Lajpat Nagar,Ghaziabad - 201005, Uttar Pradesh, India
Phone :08045813058
- Breathing Circuit and Accessories
- Airway Management
- Intubation Devices And Accessories
- Tracheostomy Tube
- Endotracheal Tube
- Anaesthesia Face Mask
- CPAP And BIPAP Mask And Accessories
- HMES And HMFS Breathing Filter
- Oxygen And Nebulization Therapy Products
- Neonatal Care Products
- Gel Positioner
- Medical Grade CSSD Products
- Catheter Kit
- Suction Tube
- Besmed NICU Care Products
- Surgical Gown
- Nasal Cannula
- Urology Products
- Infusion Pump
- Prone Head Positioner With Mirror
- Cautery Pencil
- Pulse Oximeter
- Nebulizer Machine
- Foley Catheter
- Oxygen Flow Meter
- Strile Spiral Extension Line
- Yankauer Suction Set
- CPAP System
- AIRWAY TUBE
- AMBU BEG
 Send Inquiry
Send Inquiry Send SMS
Send SMS Call Me Free
Call Me FreeMark Enterprises
All Rights Reserved.(Terms of Use)
Developed and Managed by Infocom Network Private Limited.
Developed and Managed by Infocom Network Private Limited.

